Laurie's Blogs.

Jun 2017
Mobilizing the hypermobile joint
Laurie Edge-Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT
This blog topic comes from a blog I found about whether or not it is appropriate to mobilize a painful lax ankle sprain. http://www.themanualtherapist.com/2017/04/mmt-q-should-i-mobilize-painful-lax.html
And the answer I think is interesting, and should be thought about for both humans and our canine companions.
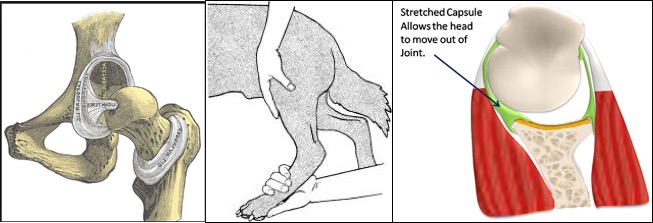
So firstly, let’s think about where pathologic laxities might occur in our canine patients: Full ACL tears; Medial Shoulder Instabilities; Carpal Hyperextension; Hip dysplasia; Lumbosacral Instabilities & Other Spinal Hypermobilities (non-surgical). Secondly, it’s important to also note that mobilizations have effects not only on mobility (i.e. stretching of tight ligamentous or fascial structures) but also on neural imputing and blood flow.
If in the case of a ‘lax’ joint, the patient (animal or human) is fearful of loading the joint (i.e. off-loading or making postural compensations), then return to function and appropriately strengthening isn’t possible. Manual therapy gives us a window into the nervous system in order to reduce fears of loading a limb (i.e. as in a full CCL tear) or moving into certain postures (i.e. extension of the lumbosacral junction in dogs with lumbosacral disc disease), or to reduce pain signaling from a joint.
A bonus is that research studies have found that mobilizations have been able to increase strength in adjacent muscles and improve limb stability (i.e. single leg standing) as well. So, mobilizing may actually affect proprioceptive awareness and balance in a limb.
Some of the real neurophysiological magic happens when joints are mobilized nearer to end range (i.e. grade 3 or 4 mobilizations). So, the original blog post states, we shouldn’t fear mobilizing into these ranges so long as there is no pain or apprehension experienced by the patient. (If there is, then stick with grades 1 - 2's.)
What would I do with each of the following scenarios?
Full ACL: Cranial and caudal glides
Medial Shoulder Instabilities: Medial and lateral glides
Carpal Hyperextension: Cranial glides of the carpal bones
Hip Dysplasia: Lateral glides
Lumbosacral Instabilities: Flexion mobilizations, Side-bend glides in flexion, & Tail pulls
Mobilizing a joint might even be best before you do exercises. Not hours of mobilizing, but perhaps 1 – 3 minutes’ worth. (Note, I spend more time on spinal mobs than I do on extremity joint hypermobilities… the affected joint itself and a couple of adjacent segments. This seems to setting things down nicely.)
And with that, Happy Mobilizing!